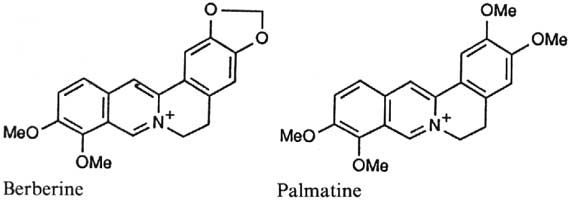
Figure 1: Berberine and palmatine.
IMPETIGO AND ITS TREATMENT
Inhibitors of Staphylococcus
Impetigo is a bacterial skin infection caused mainly by Staphylococcus aureus (in more than 90% of cases) but sometimes by group A Streptococcus, both pathogens leading to formation of pustules. The disorder primarily affects children, particularly before age 12; it can rarely occur in adults. The infection is experienced more often in warm weather and it is spread around the body from an initial localization by scratching the sores and then infecting other parts of the skin. The disease is usually treated with antibiotics, which are usually effective for an outbreak, but the condition can occur again upon exposure to the bacteria. The majority of cases occur where children are living in unclean conditions, and among those who with weakened immune function as the result of inadequate diet. The disease is related to folliculitis, boils, carbuncles, and cellulitis, all caused by Staphylococcus, and to erysipelas, caused by Streptococcus. In addition, sore, cracked nipples in breastfeeding mothers are often a type of impetigo caused by Staphylococcus aureus. Staphylococcus has also been implicated in some cases of acute dermatitis and chronic eczema.
Antibiotics and antiseptics are applied topically and/or antibiotics are given internally. For localized lesions, topical mupirocin ointment applied three times daily for ten days is the usual treatment. For more widespread infections, oral therapy with cephalexin, erythromycin, or dicloxacillin may be used. Alternative treatments are being investigated to maximize response and minimize the chances of drug side effects (mainly from oral therapies) and avoid problems of drug resistance.
In a recent study (1), a topical application of fusidic acid (an antibiotic) with povidone-iodine (iodine complexed with the polymer povidone that releases the iodine gradually) was tried. This treatment was deemed effective in attaining clinical cure of impetigo after just one week, but in only 55% of children so treated. The researcher in charge of the project was mainly interested in the use of fusidic acid as a treatment; the povidone-iodine combination is sometimes irritating and is a standard topical therapy for the disease that served as the control treatment. Fusidic acid, a steroid like molecule which does not, however, have steroid-like activity, is used for mild to moderately severe skin and soft-tissue infections, including impetigo, folicullitis, erythrasma, furunculosis, abscesses, and infected traumatic wounds. The topical combination of fusidic acid with a steroid (e.g., betamethasone or hydrocortisone) is very useful in the treatment of atopic dermatitis and eczema when staphylococcal secondary infection or staphylococcal antigen is suspected to be a contributor (5). In most cases of skin staphylococcal infection, when topical and oral routes of treatment have been studied individually and compared, the oral route has had a higher level of effectiveness and lower rate of recurrence.
Pharmaceutical researchers, especially those working in countries where herbal medicine remains of interest, have begun evaluating the potential use of herbs and their active components in the treatment of impetigo, with special emphasis on treating drug resistant strains of the bacteria that cause this disease. For example, in a clinical study of topical impetigo treatment, extract of black tea was reported to be effective for more than 80% of children treated, being as valuable as using topical framycetin and gramicidin, or oral cephalexin (2). The main active component of tea, epigallocatechin, was tested in combination with antibiotics to treat resistant strains of Staphylococcus aureus in vitro, showing good effects (6, 7). Other herb components found useful against antibiotic resistant S. aureus include carvone from star anise and benzyl benzoate from Acorus graminaeus; these compounds were tested in conjunction with antibiotics (e.g., ampicillin or chloramphenicol) to overcome the resistant strains (8). Licorice has been shown to inhibit S aureus, and its flavone components appear to be particularly active, usable against drug resistant strains (10). Staphylococcus becomes easily resistant to gentamicin and erythromycin, and, to a lesser extent, methicillin.
In China, impetigo is known as huangshi chuang (yellow-discharge sore). The disease is thought to be produced by the combination of internal damp-heat and external toxic-evil (3). Damp-heat arising internally is usually understood to be due to dietary factors, especially when the stomach/spleen function is weak and unable to distribute moisture. The accumulated dampness from fatty, moist, and salty foods, and from food residue that remains too long as a result of weak stomach function, transforms into heat, yielding the internal damp-heat condition. The external toxic-evil corresponds to the contact with the bacterial pathogen. The primary therapy is to clear heat and toxin and eliminate dampness. An example of a formula is Qinlian Pingwei Tang (Scute and Coptis Stomach Benefiting Decoction):
| Scute | 10 grams |
| Coptis | 10 grams |
| Lonicera | 10 grams |
| Forsythia | 10 grams |
| Gardenia | 10 grams |
| Chiang-huo | 10 grams |
| Alisma | 12 grams |
| Hoelen | 15 grams |
| Red Atractylodes | 10 grams |
| Dandelion | 12 grams |
| Patrinia | 15 grams |
This is taken orally as a decoction. Topically, a powder of rhubarb, phellodendron, scute, and sophora is applied with enough water to moisten it (or a skin wash can be prepared with the herbs). A similar treatment recommendation is found in the Encyclopedia of Practical Traditional Chinese Medicine (4), deleting the herbs for dampness:
| Scute | 9 grams |
| Coptis | 9 grams |
| Lonicera | 15 grams |
| Chrysanthemum | 15 grams |
| Gardenia | 9 grams |
| Phellodendron | 9 grams |
| Viola | 15 grams |
| Semiaquilegia | 9 grams |
| Dandelion | 15 grams |
The chrysanthemum to be used is wild chrysanthemum (yejuhua) and the formula is prepared as a decoction with the amounts indicated forming a one day dose. For topical therapy, a combination of lonicera, chrysanthemum, phellodendron, sophora, and alum is recommended.
Chinese reports of successful treatment of infant eczema with topical phellodendron-based treatments (11) may, in fact, represent therapy for atopic dermatitis associated with Staphylococcus. The alkaloids of phellodendron, such as berberine and palmatine (see Figure 1), have antiseptic action against Staphylococcus and Streptococcus. Coptis (see Figure 2), another source of berberine and palmatine, was shown to inhibit S. aureus, while the combination of coptis, scute, and licorice had an even stronger effect (9).
The Chinese herbs recommended for internal use are mainly those used for damp-heat (e.g., coptis, scute, phellodendron, and gardenia, the components of the well-known Coptis and Scute Combination, Huanglian Jiedu Tang) and those used for toxic heat (e.g., forsythia, lonicera, dandelion, viola, semiaquilegia, patrinia). The dosage of herbs taken internally in one day is about 100-120 grams. Topical therapies often rely on sophora and phellodendron, two herbs with broad-spectrum antibacterial properties.
March 2002
