return to itm online
REDUCING INFLAMMATION WITH DIET AND SUPPLEMENTS:
The Story of Eicosanoid Inhibition
general review by Subhuti Dharmananda, Ph.D., Director, Institute for Traditional Medicine, Portland, Oregon
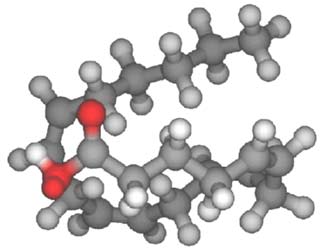
Several important diseases are mediated by production of molecules known as eicosanoids, so named because they are derivatives of the 20-carbon arachidonic acid ("eicos" is from the Greek word eikosi, the number 20; see Figure 1). These diseases include heart attack, asthma, arthritis, ulcerative colitis, asthma, dysmenorrhea, and recurrent headaches.
|

Figure 1: Arachidonic acid: three dimensional representation, top; chemical structure diagram, bottom. The molecule is a long chain of CH and CH2 units, terminated by the acid unit (COOH). There are 20 carbons in a linear chain that is folded as indicated in the 3-D representation.
|
The story of eicosanoids and their involvement in inflammation and chronic diseases is complex and rapidly evolving. Information here is necessarily simplified and is intended to help explain the basis for consuming certain foods, oil-based supplements, and herbs in an effort to prevent or help control certain diseases. The eicosanoids of concern are divided into three groupings (further subdivided by letter and number, as in PGE1, based on the structural features of the molecule: see Figures 2 and 3 for chemical structure diagrams and Tables 1 and 2 for individual eicosanoid effects):
- prostaglandins (PG): primarily have the effects of influencing platelet aggregation (inhibiting or increasing) and constricting or relaxing blood vessels. Some prostaglandins have favorable effects, such as insuring the integrity of the gastric lining, regulating kidney function, and initiating some stages of childbirth, but many produce negative effects, such as intensifying pain, causing cramping, and restricting blood circulation. PGE2 is one of the main prostaglandins involved in inflammation.
- thromboxanes (TX): are produced by platelets; they enhance platelet aggregation and also cause constriction of blood vessels and bronchioles. Thromboxanes are mostly known for their negative impact, particularly on cardiovascular health (TXB) and also as contributor to asthma (TXA), but they may play a role in the immediate response to injury, to limit blood loss.
- leukotrienes (LT): are produced by immune system cells and stimulate production of immune system signaling molecules such as interleukins (IL), interferon (IFN), and substances involved in anaphylactic reactions. Leukotrienes are mostly known for their contribution to allergies and autoimmune diseases.
There are other, less well-studied eicosanoids (e.g., such as those known as HETEs and EETs and lipoxins, all these being closely related to the leukotrienes). The process yielding inflammation and/or more severe disease symptoms begins with a stimulus (e.g., injury, infection, autoimmune trigger) that produces increased cellular cAMP, promoting production of the eicosanoids. This initiation process is followed by a cascade of events involving responses to these eicosanoids, potentially yielding fluid exudation, circulatory changes, increased pain sensitivity, and other manifestations of the disease. While inflammatory responses to acute infections and injuries mediated by these eicosanoids have certain beneficial effects, persistent inflammation has a degrading effect that can lead to debility and death.
Figure 2: Prostaglandins and thromboxanes. Prostanoic acid is the basic prostanoid molecule,
and the ring structure (top) varies to yield the different groups of prostaglandins and thromboxanes (bottom).
These are all formed from arachidonic acid by the action of the COX enzymes.
Figure 3: Leukotrienes; these are formed from arachidonic acid by action of the LOX enzymes.
EICOSANOID PRODUCTION
Eicosanoids are produced primarily from arachidonic acid that has been released from cell membrane phospholipids by the action of the enzyme phospholipase-A2. This enzyme is routinely present to participate in the maintenance of the cell membranes, but is induced in larger amounts by the triggers that are involved in initiating or maintaining inflammation. Release of arachidonic acid by phospholipase-A2 can be inhibited by the action of corticosteroid drugs.
Most drug treatments for diseases that involve painful inflammation block the production of eicosanoids after arachidonic acid has already formed (see Figure 4 for site of action diagram). The most frequently used drugs inhibit the cyclooxygenase enzymes (COX). This is understood to be one of the main roles of the over the counter non-steroidal anti-inflammatory drugs (NSAIDS), such as aspirin, acetaminophen, and ibuprofin.
There are several cyclooxygenases, of which COX-1 and COX-2 are most intensively studied (a third, COX-3, is under investigation). Although there are some caveats to this statement, the general view is that inhibiting COX-2 reduces inflammation, while inhibiting COX-1, which can also inhibit inflammation, produces many of the undesired side effects of the drugs (by blocking production of desirable prostaglandins, thus causing gastric damage and, with prolonged use of high doses, renal toxicity). This interpretation arises because COX-1 enzymes are produced in most of the body tissues and are present all the time, helping maintain homeostasis, while COX-2 is present in more limited quantity and in only some tissues, but appears in large amounts in response to inflammation triggers (COX-2 induction is inhibited by corticosteroid drugs). So, a recent area of drug development (since 1990, with drugs appearing in 1999) has been with inhibitors that target COX-2, but leave COX-1 uninhibited. The COX enzymes are involved in producing both PGs and TXs (these two groups of cyclic eicosanoids are called prostanoids). Unfortunately, it turns out that blocking COX-2 strongly and for a prolonged period, can still have adverse effects by inhibiting some desirable byproducts of its action and by diverting arachidonic acid metabolism to production of undesirable leukotrienes (and HETEs). COX-2 inhibitors have fewer gastric side effects than general COX inhibitors, but still have them; they may also produce undesirable cardiovascular side effects. All of the drugs blocking prostanoid synthesis from arachidonic acid are usually preferred over the more powerful steroids because of undesirable systemic effects of the steroids.
Most recently, much interest has focused on LOX (lipoxygenase) inhibitors that mainly block leukotriene synthesis. There are three main LOX enzymes that are known to be involved in the leukotriene pathway, 5-LOX, 12-LOX, and 15-LOX. Most attention has focused on 5-LOX, which appears to be the key enzyme when it comes to blocking leukotriene synthesis. For many diseases, especially those with a basis in autoimmune processes, where immune cells are intimately involved, inhibiting the prostanoids is not sufficient to give relief. For asthma, where constriction of the bronchioles is the trigger to an attack, LOX inhibitors are a critical method of therapy and this application is the first one for drug development (leukotrienes induce bronchiospasm; prostaglandin inhibitors, such as aspirin, can induced asthma attacks, perhaps by leaving more arachidonic acid available for the LOX enzymes). Ideally, one would like to be able to inhibit both COX-2 and 5-LOX simultaneously, to maximize anti-inflammatory effects. Thus, drug researchers are now intensively seeking compounds of low toxicity that block COX-2 and 5-LOX.

Figure 4: Steps in the biosynthesis of eicosanoids where different drugs have their effects
(the usual NSAIDs are COX inhibitors; LOX inhibitors are NSIADS of a new type).
TABLE 1. Properties of Significant Eicosanoids. Some eicosanoids affect immune messengers called interleukins (ILs; especially IL-1α and IL-2) and interferon-gamma (INF-γ).
| Eicosanoid
| Major Site(s) of Synthesis
| Major Biological Activities
|
| PGD2
| mast cells
| inhibits platelet and leukocyte aggregation, decreases T-cell proliferation and lymphocyte migration and secretion of IL-1Α and IL-2; induces vasodilation and production of cAMP
|
| PGE2
| kidney, spleen, heart
| increases vasodilation and cAMP production, enhancement of the effects of bradykinin and histamine, induction of uterine contractions and of platelet aggregation; decreases T-cell proliferation and lymphocyte migration and secretion of IL-1Α and IL-2
|
PGF2α
| kidney, spleen, heart
| increases vasoconstriction, bronchoconstriction and smooth muscle contraction
| |
| PGH2
| many sites
| a short-lived precursor to thromboxanes A2 and B2, induction of platelet aggregation and vasoconstriction
|
| PGI2
| heart, vascular endothelial cells
| inhibits platelet and leukocyte aggregation, decreases T-cell proliferation and lymphocyte migration and secretion of IL-1Α and IL-2; induces vasodilation and production of cAMP
|
| TXA2
| platelets
| induces platelet aggregation, vasoconstriction, lymphocyte proliferation and bronchoconstriction
|
| TXB2
| platelets
| induces vasoconstriction
|
| LTB4
| immune cells*
| induces leukocyte chemotaxis and aggregation, vascular permeability, T-cell proliferation and secretion of INF-&gamma , IL-1 and IL-2
|
| LTC4
| immune cells*
| component of SRS-A**, induces vasodilation, vascular permeability and bronchoconstriction and secretion of INF-&gamma
|
| LTD4
| immune cells*
| predominant component of SRS-A, induces vasodilation, vascular permeability and bronchoconstriction and secretion of INF-&gamma
|
| LTE4
| mast cells and basophils
| component of SRS-A**, induces vasodilation and bronchoconstriction |
* mainly from immune cells, such as monocytes, basophils, alveolar macrophages, neutrophils, eosinophils, mast cells, epithelial cells;
** SRS-A = slow-reactive substance of anaphylaxis
TABLE 2. Physiological Effects of Prostanoids.*
| Affected Part
| Effects of Specific Prostanoids
|
| Vascular smooth muscle
| PGEs & PGI2 → smooth muscle dilation → vasodilation
PGF2a & TXA2 → vasoconstriction
|
| GI tract smooth muscle
| PGI2, PGF2 & PGI2 → smooth muscle contraction → cramps
PGE → decreased gastric acid secretion & ulceration
|
| Lung smooth muscle
| PGI2 & PGE2 → vasodilation & constriction, respectively
TXA2 is a vasoconstrictor & bronchoconstrictor
PGFs contract while PGEs relax respiratory smooth muscle
|
| Platelets
| PGE1 & PGI2 → decreased platelet aggregation
TXA2 → increased platelet aggregation
|
| Reproductive organs
| PGE2 & PGF2a → uterine contractions
initiate & stimulate labor; menstrual pain
|
| Kidneys
| PGE regulates arteriolar tone, compensatory vasodilatation, maintains normal blood flow, increased glomerular filtration rate
|
| Inflammatory processes
| fever: PGEs act on thermoregulatory center in brain → increased body temperature
pain: PGs → sensitize pain receptors to stimulation → increased pain
PGs promote vasodilation & increased vascular permeability
|
*Note: The other eicosanoids, leukotrienes (LTs), are less fully researched and more consistent in their actions than the prostaglandins and thromboxanes. All LTs are extremely potent smooth muscle contractors. LTB4 promotes white blood cell adherence, chemotaxis & degranulation. LTC4 , LTD4 & LTE4 promote increased vascular permeability, plasma exudation & mucus secretion. LTs also promote bronchoconstriction and vasoconstriction; they decrease myocardial contractility and coronary blood flow.
DIET, EICOSANOIDS, AND INFLAMMATION
Even if drug therapy successfully blocks the COX and LOX enzyme systems, arachidonic acid can still be converted into other damaging molecules, such as epoxy derivatives. So, another approach to treating the diseases involving eicosanoids seems desirable: to try to prevent eicosanoid production by dietary modifications. Not all of the phospholipids in cell membranes include arachidonic acid, only those that were derived from certain dietary fatty acids, mainly linoleic acid. The concept of dietary control over these diseases is based, in part, on starving the eicosanoid system by reducing the fatty acids (specifically, the polyunsaturated fatty acids, PUFAs) that can eventually make arachidonic acid, thereby slowing down the production of eicosanoids when a stimulus occurs.
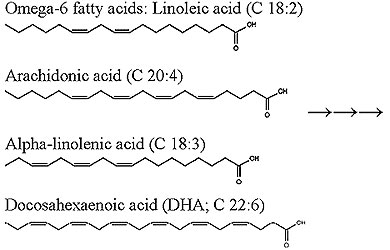
Two main fatty acid groups are considered in relation to this dietary approach: one is the omega-6 fatty acids, which become phospholipids readily converted into arachidonic acid, and other is omega-3 fatty acids, which become phospholipids that are not as easily converted to arachidonic acid (they become, instead EPA and DHA; see Figure 5). The difference between omega-3 and omega-6 fatty acids is the location of double bonds in the hydrocarbon chain.
The dietary approach requires learning the fatty acid profile of food oils (see Table 3) in order to shift from one high in omega-6 fatty acids (which is the normal condition for most diets) to one high in omega-3 fatty acids. As can be seen in Table 3, if one is seeking to consume a high proportion of omega-3 fatty acids compared to omega-6 fatty acids, there are very few oils that are especially favorable. Oils that are considered beneficial in other contexts (e.g., olive oil, non-animal oils, wheat germ oil, etc.) do not present a favorable fatty acid ratio (they may have less saturated fats and contain other beneficial constituents). Of the food materials listed, only fish provide a significant omega-3 profile and do so with both short chain and long chain fatty acids. Fish oil provides a second benefit, in that it reduces T-cell stimulation in the intestinal tract that may be involved in triggering inflammation and auto-immune responses.
Perilla seed oil and flax seed oil are usually obtained as dietary supplements, not used as foods. Canola oil, which has become a mainstay of the food product manufacturing industry, is considered valuable because it has low saturated fat, a relatively favorable omega-3/omega-6 ratio (the best of the readily available vegetable sources), and is easy to get and inexpensive. Olive oil, considered amongst the most healthful, contains a relatively large amount of oleanolic acid, which may help block eicosanoid production; it can have a favorable effect, but not by providing large amounts of omega-3 fatty acids.
| 
|
Figure 5. Right: enzyme action on dietary oils: production of arachidonic acid from omega-6 fatty acids; omega-3 fatty acids yield, instead, eicosapentaenoic acid (EPA), which is further metabolized to form docosahexaenoic acid (DHA). Left: the basic dietary omega-6 fatty acid (linoleic acid) and its product arachidonic acid; the basic plant-based omega-3 fatty acid and its product of metabolism, DHA, which, like EPA, is obtained directly from fish oil. The molecules are labeled according to the number of carbons and number of double bonds in the chain.
|
TABLE 3. Fatty Acids of Food Oils in Descending Rank by Short Chain Omega-3/Omega-6 Ratio.
The oils have been subdivided by categories, but the list order for all oils is by omega-3/omega-6 rank, not just by category. The data shown indicates parts per million (ppm) of the component in the oil. These oils provide about 120 calories (kilocalories) per tablespoon. Long chain (20 and 22 carbon) fatty acids are almost exclusively found in fish oils; the long chain omega-3 fatty acids in fish are EPA (20-carbon) and DHA (22- carbon). Data were provided by the National Institutes of Health.
|
Food Oil Identity and Specification
|
18-carbon
|
20- & 22-carbon
|
Short 6
| Short 3
| Long 6
| Long 3
|
|
Herbal Oils: Selected for High Omega-3 Fatty Acid
Content
|
| Perilla seed oil |
1680
| 8960
| 0
| 0
|
| Flaxseed oil |
2240
| 7980
| 0
| 0
|
|
Fish Oils: High in Long-Chain Omega-3 Fatty Acids
|
| Fish oil, herring |
156
| 417
| 39
| 1509
|
| Fish oil, salmon |
210
| 525
| 92
| 4657
|
| Fish oil, sardine |
274
| 592
| 239
| 3096
|
| Fish oil, cod liver |
127
| 254
| 127
| 2557
|
| Fish oil, menhaden |
293
| 575
| 159
| 3624
|
|
Miscellaneous Oils with at Least 10% Omega-3
|
| Butter oil (ghee; moisture removed) |
288
| 185
| 0
| 0
|
| Oil, canola |
2842
| 1302
| 0
| 0
|
| Oil, mustard |
2146
| 826
| 0
| 0
|
| Oil, walnut |
7194
| 1414
| 0
| 0
|
| Oil, soybean |
6936
| 925
| 0
| 0
|
| Oil, soybean lecithin |
5465
| 698
| 0
| 0
|
| Oil, wheat germ |
7453
| 938
| 0
| 0
|
| Shortening, household, lard + vegetable oil |
1242
| 141
| 0
| 0
|
|
Miscellaneous Oils with Considerably Less than 10%
Omega-3
|
| Oil, olive |
1067
| 81
| 0
| 0
|
| Oil, soybean (hydrogenated; margarine) |
4746
| 354
| 0
| 0
|
| Mayonnaise, soybean and safflower oil |
7176
| 414
| 0
| 0
|
| Shortening, industrial, lard + vegetable oil |
2317
| 128
| 0
| 0
|
| Oil, sunflower > 70% oleic |
505
| 27
| 0
| 0
|
| Oil, rice bran |
4542
| 218
| 0
| 0
|
| Margarine-butter blend |
2162
| 103
| 0
| 0
|
| Oil, palm |
1238
| 27
| 0
| 0
|
| Oil, corn |
7888
| 95
| 0
| 0
|
| Oil, sesame |
5617
| 41
| 0
| 0
|
| Oil, sunflower, linoleic < 60% |
5413
| 27
| 0
| 0
|
| Oil, cottonseed |
7004
| 27
| 14
| 0
|
| Oil, grapeseed |
9466
| 14
| 0
| 0
|
|
Miscellaneous Oils with no Detectable Omega-3
|
| Oil, peanut |
4320
| 0
| 0
| 0
|
| Oil, coconut |
245
| 0
| 0
| 0
|
| Oil, sunflower, linoleic > 60% |
8935
| 0
| 0
| 0
|
| Oil, palm kernel |
218
| 0
| 0
| 0
|
The idea of adjusting the diet and taking supplements to control eicosanoid-based diseases is a popular one amongst some proponents of natural health care, and there is considerable research supporting the approach, but it must be viewed in proper context. Fats in a healthy diet comprise about 30% of the daily caloric intake, and it is recommended that polyunsaturated fatty acids make up about 10% of the caloric intake. This corresponds, roughly to 150 grams of PUFAs per week. What contribution will be made from eating fish and taking supplements?
The fish with the highest levels omega-3 fatty acids are listed in Table 4. If a person consumes 1 pound of fish per week, this provides about 2-10 grams of omega-3 fatty acids. If one additionally takes encapsulated oils, either from plant sources or fish, the usual dosing is about 3 grams of oil per day. Up to 2/3 of the supplement oil may be omega-3 fatty acids (mainly as EPA and DHA in the fish oil), so up to 14 grams per week can be obtained from taking capsules. Together, these measures might contribute about 10-15% of one's total PUFA intake. To further assure a good level of omega-3 versus omega-6 fatty acids, one would minimize consumption of oils that are at the bottom Table 3. When consuming meats, preference should be given to those from grass-fed animals rather than corn-fed animals, as the meat of the former will have some omega-3 fatty acids, while the latter will not (corn provides almost no omega-3 fatty acids).
TABLE 4. Examples of Fish with High Levels of Fats and Omega-3 Fatty Acids.
Amounts shown are percent of the uncooked fish, as presented typically in shops.
| Fish
| % Total Fat
| % Omega-3 Fatty Acids
|
| Pollack
| 1.0
| 0.4
|
| Halibut
| 2.3
| 0.4
|
| Striped bass
| 2.3
| 0.8
|
| Smelt
| 2.4
| 0.7
|
| Rainbow trout
| 3.4
| 0.6
|
| Swordfish
| 4.0
| 0.6
|
| Bluefish
| 4.2
| 0.8
|
| Freshwater catfish
| 4.3
| 0.4
|
| Bluefin tuna
| 4.9
| 1.2
|
| Salmon (Atlantic)
| 6.3
| 1.4
|
| Albacore tuna
| 7.2
| 2.1
|
| Lake trout
| 9.4
| 1.4
|
| Chinook salmon
| 10.4
| 1.4
|
| Mackerel (Atlantic)
| 13.9
| 2.3
|
| Herring (Atlantic)
| 18.0
| 1.6
|
Over the long term, with years of following such a regimen of eating fish and/or using favorable vegetable oils and taking supplements, while reducing omega-6 rich foods, certain health benefits can be expected (statistically) because of the lower production of eicosanoids. In areas where fish consumption is high, such as Japan, Greenland, and the areas bordering the Mediterranean Sea, the population ingests a considerably higher proportion of omega-3 fatty acids than in other areas where there is little fish consumption, and the measured risk for death by cardiovascular diseases is decreased. This indicates that years of eating such a diet may reduce the vasoconstriction, platelet aggregation, and chronic arterial inflammation that lead to heart attacks and stroke. Similarly, it is believed that such diets can reduce the incidence of certain cancers, such as prostate cancer and colon cancer, by a similar mechanism of reducing adverse eicosanoid effects.
By contrast, attempting to strongly control inflammation in acute manifestations such as asthma and arthritis by diet alone becomes much more difficult. Not only is it difficult to get adequate quantities of omega-3 fatty acids to resolve the acute condition (since omega-6 fatty acids are still so prevalent), but excessive use of omega-3 fatty acids, via supplementation, may have undesired effects. At high levels, these fatty acids may produce an undesired level of immune suppression and they serve as pro-oxidants (which can be partly countered by consuming antioxidants in the diet, such as those in tea, fruits, and vegetables, or taking additional supplements, such as vitamins C and E). To have a strong favorable impact in a short time, a more dramatic change in eicosanoid production may be needed, attained by limiting production of eicosanoids from arachidonic acid.
BLOCKING OF COX AND LOX ENZYMES BY NATURAL THERAPIES
Certain herbs (and individual active ingredients from herbs, see Appendix for the example of PCTs) inhibit the COX and/or LOX enzymes at dosages that can be appropriate for oral consumption. These may serve as alternatives to drugs, especially for milder forms of the eicosanoid-dependent diseases. Some of them are being used clinically, such as curcumin, boswellic acid, oleanolic acid, allicin, berberine, and the tea catechins. As this research is intensively being pursued, any list of potential agents is incomplete. Examples of herb ingredients with eicosanoid inhibitor activities are provided in Tables 5 and 6, modified from lists developed by Dr. James Duke.
TABLE 5. Sample Plant Constituents with Cox-2 Inhibitor Activity.
The substances listed here have been subjected to in vitro testing with effective concentrations determined. When possible, these concentrations are given in terms of IC50 (the inhibition concentration that yields a 50% inhibition of the enzyme). As a reference, the drug indomethacin has an IC50 of 1 uM. The lower the IC50 value, the more potent the compound. Units of measurement are either micromolar (uM) which takes into account the molecular weight of the substance, and micrograms/milliliter (ug/ml), which only takes into account the weight of the substance.
| Substance
| Sample Plant Source
| Inhibitor Activity Measure
|
| Apigenin
| tea, numerous sources
| <40 uM
|
| Baicalein
| scute (huangqin)
| 100 ug/ml
|
| Berberine
| phellodendron (huangbai)
| 100 ug/ml
|
| Curcumin
| turmeric (jianghuang)
| 10 uM
|
| Eicosapentaenoic acid
| garlic (dasuan)
| 1 uM
|
| Evodiamine and evodol
| evodia (wuzhuyu)
| 2.5 ug/ml
|
| Oleanolic acid
| numerous
| IC50 = 295 uM
|
| Quercetin
| numerous
| <40 uM
|
| Resveratrol
| hu-chang (huzhang)
| 30 uM, 50 uM, >2.5->22.5 uM
|
| Rutaecarpine
| evodia (wuzhuyu)
| 2.5 ug/ml
|
| Ursolic acid
| ligustrum (nuzhenzi)
| IC50 = 130 uM
|
TABLE 6. Sample Plant Constituents with Lox-Inhibitor Activity.
| Constituent
| Sample Plant Source
| Inhibitor Activity Measure
|
| Allicin
| garlic (dasuan)
| D = 25 ug/ml
|
| Berbamine
| hu-chang (huzhang)
| IC50 = 40 uM
|
| Berberine
| coptis (huanglian), phellodendron (haungbai)
| IC50 = 118 uM
|
| Boswellic acid
| frankincense (ruxiang)
| IC50 = 1.5 uM
|
| Caffeic acid
| taraxacum (pugongying)
| IC50 = 62-148 uM
|
| Epicatechin
| tea
| IC50 = 140 uM
|
| Epicatechin-gallate
| tea
| IC50 = 18 uM
|
| Epigallocatechin
| tea
| IC50 = 21 uM
|
| Fisetin
| chih-shih (zhishi)
| IC50 = 11 uM
|
| Flavone
| numerous
| IC50 = 32 uM
|
| Galangin
| galanga (liangjiang)
| IC50 = 20 uM
|
| Morin
| morus (sangbaipi)
| IC50 = 160 uM
|
| Quercetin
| numerous
| IC50 = 0.1-5 uM
|
| Theaflavin digallate
| tea
| IC50 = 0.25 uM
|
| Ursolic acid
| ligustrum (nuzhenzi)
| IC50 = 180 uM
|
SUMMARY AND SUGGESTIONS
There is no doubt that inhibiting eicosanoid synthesis by modern drugs therapies is effective for many people in reducing the inflammation and the accompanying pain of many diseases, particularly arthritis. It has been shown that regular consumption of aspirin, even in small doses of about 80 mg/day, reduces risk of heart attack and colon cancer, and this effect appears to be mediated, at least in part, by inhibiting eicosanoids. For those suffering from serious diseases, many wish to avoid using the standard drugs, or avoid using them frequently, due to experience of side effects or concerns about side effects. Prolonged use of corticosteroid drugs and NSAIDS has been linked to serious reactions in some individuals. In order to take reasonable steps to minimize the symptoms of these diseases through means other than relying on the drugs, it is important to understand the process by which the inflammation and other disease manifestations (e.g., platelet sticking, bronchiospasms) occur.
Detailed analysis of the pathways to inflammation indicate that linoleic acid, the basic omega-6 fatty acid, is transformed into arachidonic acid, which is incorporated into phospholipids making up all cell membranes. A stimulus then returns the phospholipid to arachidonic acid, which is metabolized by certain enzymes (mainly COX and LOX) into prostaglandins, thromboxanes, and leukotrienes that are critical to yielding various disease manifestations, including constriction of blood vessels and bronchioles, changes in platelet function, and development of inflammation. Two basic means of interrupting this pattern seem evident:
- Avoid producing arachidonic acid by ingesting less linoleic acid and, instead, load the membranes with phospholipids derived from omega-3 fatty acids, so that the initial stimulus to inflammation produces less arachidonic acid.
- Inhibit the enzymes (e.g., COX and LOX) involved in the production of the eicosanoids from arachidonic acid. This is the function of modern drug therapies, including steroids and non-steroid drugs, but can also be a goal of herbal therapies.
To load the body with omega-3 fatty acids in place of omega-6 fatty acids, one can consume oily fish (with salmon, albacore tuna, and sardines being palatable and readily available options) in place of other foods (e.g., corn-fed beef), and rely on food oils that have a higher ratio of omega-3 to omega-6 fatty acids than might normally be consumed. The main food oils (readily available and commonly used) with somewhat favorable fatty acid profiles are butter, canola oil, and soy oil. The food sources can be supplemented by specially-prepared oils, usually made available in capsules. The primary supplements with omega-3 fatty acids are perilla seed oil, flax seed oil, and fish oil.
One should be careful, however, not to rely excessively on these oil sources for a prolonged period, particularly the herbal supplements, as they may be missing beneficial components that can be obtained from other dietary oils and the herbal oils might contain some ingredients that are not beneficial with long-term use. Even when dietary changes are made and supplements are taken to increase omega-3 fatty acids, there are still plenty of dietary omega-6 fatty acids to contribute to the process of inflammation, because so much of the naturally-occurring oils in foods are of the omega-6 type (these are usually the majority component). Still, the changes in diet and use of supplementary oils may reduce the severity of the inflammatory response sufficiently to reduce drug therapies.
Inhibiting enzymes that produce eicosanoids from arachidonic acid is still of interest for those who can pursue the route of improving the balance of ingested oils. Drinking tea and consuming garlic (with food or in capsules or tablets) is a simple method of providing some inhibition of the COX and LOX enzymes (with other favorable effects expected from these dietary components). Curcumin (from turmeric), quercetin (from numerous sources; dietarily it is mainly obtained from onions, applies, fruit juices, and tea, supplements are often derived from eucalyptus), and boswellic acid (from frankincense), are apparently safe methods of getting these enzyme inhibitors. Researchers are also actively seeking other natural LOX inhibitors. Particularly promising are branched chain fatty acids, mainly 12-MTA and 13-MTA (methyltetradecanoic acid); these are potent inhibitors of the 5-LOX enzyme. Ursolic acid, a component of several herbs used in Chinese medicine, is a moderately strong inhibitor of both COX-2 and 5-LOX (see the Appendix).
There is growing evidence that dietary factors can influence diseases, particularly in terms of lowering risk over an extended period of time. People who consume more fish, fruits, vegetables, and tea, have been shown in various studies to have a lower incidence of several serious diseases. Many fruits and vegetables provide flavonoids that may be inhibitors of inflammatory eicosanoids. Many of the substances listed in Tables 5 and 6 are flavonoids (or modified flavonoids, such as polyphenols). There can be many contributing factors to yield health benefits from these dietary components, not just reduced eicosanoid production.
Relatively high doses of effective herb components (comparable to doses of over-the-counter NSAIDS, which are typically taken in the range of several hundred milligrams per dose) may be useful in reducing acute inflammation by significantly blocking eicosanoid production. These dosages are not easily obtained in convenient form without using concentrated extracts of the herbs. Thus, the complete natural regimen for reducing inflammatory eicosanoid production includes dietary changes and use of supplements that include oils (rich in omega-3 fatty acids) and herb extracts that reduce arachidonic acid metabolism.
APPENDIX. Pentacyclic Triterpenes (PCTs) as Inhibitors of Inflammation
Pentacyclic triterpenes (PCTs) are a subdivision of an important group of botanical active constituents known as triterpenoids; when complexed with sugar molecules PCTs are called triterpene glycosides, or saponins. Several of the PCTs have inhibitory action for the COX and/or LOX enzymes. Two of the most widely occurring and intensively investigated pentacyclic triterpenes are ursolic acid and its isomer oleanolic acid; their chemical formulas are identical, and their structures differ only by the location of a methyl group (CH3), as displayed at the top of the structure diagrams below (Figure 6). These substances are of considerable interest for potential health benefits, including protective effects against development of cancer, inhibition of existing tumor cells, protection against chemotherapy and radiation therapy adverse effects, anti-inflammatory activity, antioxidant activity, cardiovascular protective effects, and antiviral effects. Several medicinal herbs that contain oleanolic acid, such as ligustrum, forsythia, and swertia, are remedies employed in China and Japan for the treatment of hepatitis. Isolated oleanolic acid has already been used in China as a treatment for hepatitis for many years. Ursolic acid is known for its ability to inhibit skin inflammation; in Japan it is also used as a topical protectant against skin cancer.

Figure 6: Ursolic Acid (left), Oleanolic Acid (right).
These compounds are synthesized in plants from squalene, a compound in which there are no closed carbon rings, but which has the basis for developing five ring (pentacyclic) compounds. Ursolic acid was named after the herb Uva Ursi (bearberry; urs is the root term for bear). Oleanolic acid was named for the olive (olea is the root term for olive), which is rich in this compound; there is a plant family called the Oleanaceae, whose members usually contain oleanolic acid. In general, plants that contain ursolic acid also contain oleanolic acid and vice versa.
| Ursolic acid and oleanolic acid form a waxy coating that is found on some plant leaves and fruits. For example, Ligustrum trees (in the Oleanaceae family) are commonly called wax trees because of these components. Ursolic acid is one of the main waxy components on apples that contributes to the smooth, shiny appearance (not to be confused with waxes sometimes added to aid storage of fruits). Squalene (left) is found in some foods, mainly concentrated in oils, such as olive oil, wheat germ oil, and bran oil (about 0.5% of the oil). The most abundant source of squalene is the liver of deep sea sharks (up to 85% squalene in liver oil). Squalene from shark livers is sold in capsules as a dietary supplement that is claimed by proponents to enhance immune functions and reduce inflammation.
|
The pentacyclic triterpenes are subdivided into several groups, such as the following:
Oleanane: oleanolic acid, ginsenosides (glycoside form), fusidic acid;
Ursane: amyrin, ursolic acid, asiatic acid, boswellic acid; and
Lupane: lupeol, betulin, betulinic acid
Of these, PCTs other than oleanolic and ursolic acid that have received considerable attention are boswellic acid (from frankincense, the resin of Boswellia serrata); asiatic acid (from gotu kola, the aerial part of Centella asiatica), and betulinic acid (from birch trees, the bark of Betula spp.). Their pharmacology is similar to that of oleanolic and ursolic acid. For example, all are being investigated for anti-inflammatory and potential anticancer effects.

Boswellic acid
SOURCES OF OLEANOLIC AND URSOLIC ACID
Chinese natural products manufacturers are now making high concentrations of oleanolic acid and ursolic acid for formulation in various internal and topical remedies. The technical extracts contain from 25% to 99% pure compound. By contrast, standard herb extracts (e.g., hot water extracts) have up to 2.0-2.5% of ursolic or oleanolic acid (commonly obtained from holy basil, Ocimum sanctum, a common ingredient in Ayurvedic formulas). Plants rich in ursolic acid include Greek sage (Salvia triloba), oleander, rosemary, lavender, and thyme (each having at least 1% ursolic acid in the leaf or whole plant)
DOSAGE
Clinical use of ursolic acid as an isolate is new, but oleanolic acid, which is nearly identical in structure but apparently milder in action, has been used for some time. Effective daily doses of oleanolic acid, based on its application in treatment of hepatitis, are reported in the range of 75-300 mg/day. For a standard dried hot water extract of an herb, which may contain about 2% of the PCTs, that dosage corresponds to use of about 4-15 grams of the extract, a large amount. Additional information on dosage of compounds of this type (see: Platycodon and other herbs with triterpene glycosides) indicates that a daily dose of about 300 mg is safe and potentially useful for long term applications and 600 mg is safe at least for short term dosage. Dr. Acharan Narula describes use of 300-500 mg or oleanolic acid as an intestinal anti-inflammatory and recommends Olenoate, a product of oleanolic acid in capsules of 100 mg each. For ursolic acid, in vitro studies have shown that it is about twice as effective as an anti-inflammatory compared to indomethacin, a potent NSAID that is administered in doses of just 50-100 mg/day; however, when converted to actual human use, the dose of ursolic acid needed may prove higher. Boswellic acid, another PCT that inhibits 5-LOX, and is used as an anti-inflammatory for arthritis, Crohn's disease, and asthma, is administered in doses of 400 mg 3 times a day of an extract standardized to contain 37.5% boswellic acids, which corresponds to 450 mg/day of boswellic acid. In general, the PCT dosage for anti-inflammatory effects appears similar to the dosage of NSAIDS.
May 2003